Pathology of COM subtypes

Inactive mucosal COM:
This condition involves dry cental perforation of pars tensa. In these patients there is permanent perforation of pars tensa. Middle ear mucosa and mucosal lining the mastoid cavity are not inflammed. The mucocutaneous junction is usually located at the margin of the perforation can extend up to the fibrous annulus.
Active mucosal COM (Perforation with otorrhoea):
In this category there is chronic inflammation of mucosa of the middle ear cavity and mastoid. Mucosa of middle ear cleft show varying degrees of oedema, submucosal fibrosis, hypervascularity and presence of inflammatory infiltrate that include lymphocytes, plasma cells and histiocytes. There is also associated increase in the number of goblet cells. Basal cell layer of middle ear mucosa also shows evidence of hyperplasia. Granulation tissue can occur and is described as aural polyp. It protrudes through the perforated ear drum.
In some areas with active COM (in both mucosal and cholesteatomatous subtypes) demonstrate focal areas of cholesterol granuloma formation. Cholesterol granuloma microscopically consists of a giant cell reaction surrounding cholesterol clefts.
Chronic inflammation is known to affect the entire middle ear cleft which include middle ear cavity proper, eustachean tube, aditus and antrum. During surgery granulation tissue from middle ear cavity, aditus, and antrum should be cleared. Active mucosal COM can cause destruction of ossicles of middle ear cavity. Ossicles show areas of hyperemia, proliferation of capillaries and formation of granulation tissue. Long process of incus commonly gets eroded because of its precarious blood supply, next to get affected would be the crura of stapes. Bacteria may also play a role in ossicular destruction especially in patients with cholesteatoma. Pseudomonas aeruginosa are known to cause destruction of ossicles by stimulating the inflammatory process.
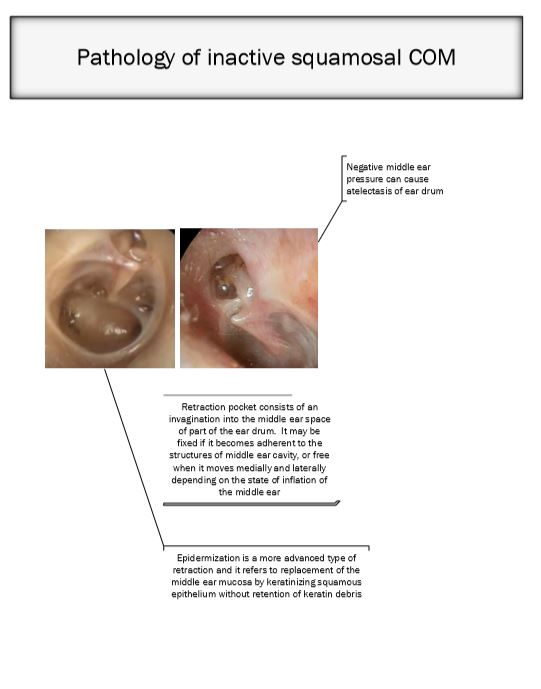
Inactive squamous epithelial COM (Retraction, atelectasis and epidermization):
In this category of COM there is negative static middle ear pressure which is followed by retraction of ear drum (atelectasis). This retraction pocket consists of invaginated ear drum into the middle ear cavity. In fact a portion of this invagination could also be adherent to the structures of middle ear. If free of middle ear structural attachement ear drum moves freely on pneumatic otoscopy, if attached the mobility of ear drum could be restricted or absent.
Epidermization is advanced stage of this retraction process and it causes replacement of entire middle ear mucosa by keratinizing squamous epithelium, but without retention of keratin debris.
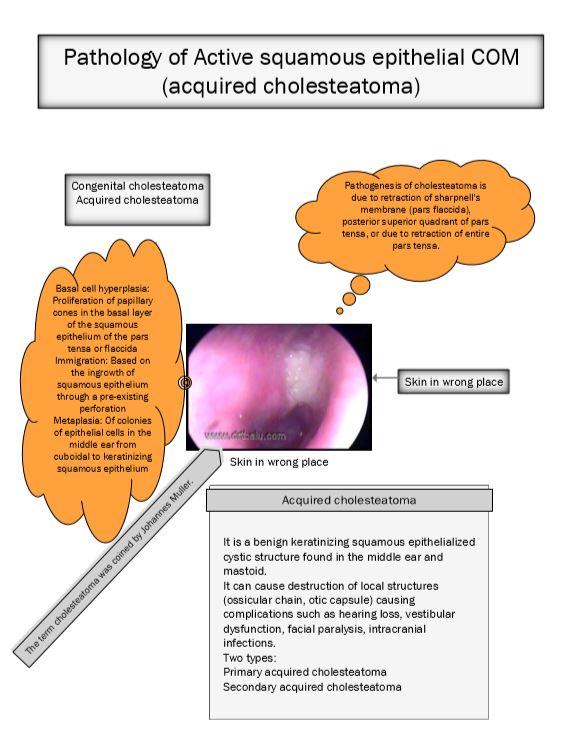
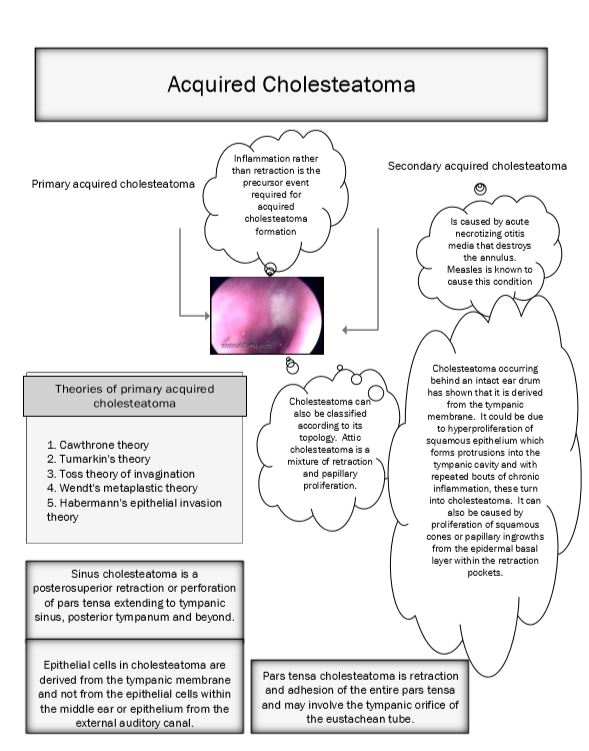
Active squamosal COM (Acquired cholesteatoma):
Cholesteatoma is defined as a cystic bag like structure lined by stratified squamous epithelium on a fibrous matrix. This sac contains desquamated squamous epithelium. This sac is present in the attic region. Cholesteatoma is also defined as 'skin in wrong place'. Cholesteatoma is known to contain all the layers of skin epithelium. The basal layer (germinating layer) is present on the outer surface of cholesteatoma sac in contact with the walls of the middle ear cleft. (This ofcourse is a old definition). This does not take into account the existence of pars tensa cholesteatoma where there is no retraction pocket as seen in pars flaccida cholesteatoma.
Cholesteatoma can cause destruction of local structures like ossicular chain, otic capsule leading on to complications like hearing loss, vestibular dysfunction, facial paralysis and intracranial disease / infection. The term cholesteatoma was first coined by the German Physiologist Johannes Muller in 1838.
Pathogenesis of cholesteatoma is due to retraction of pars flaccid or the posterior superior quadrant of pars tensa or retraction of entire pars tensa.
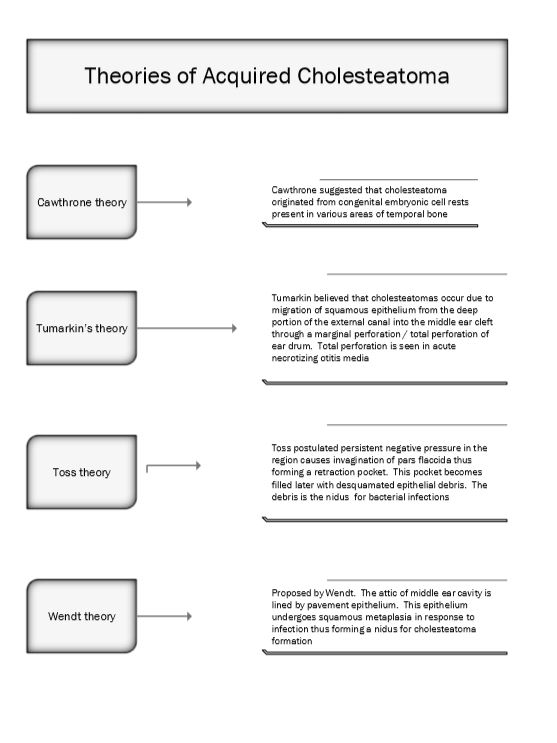
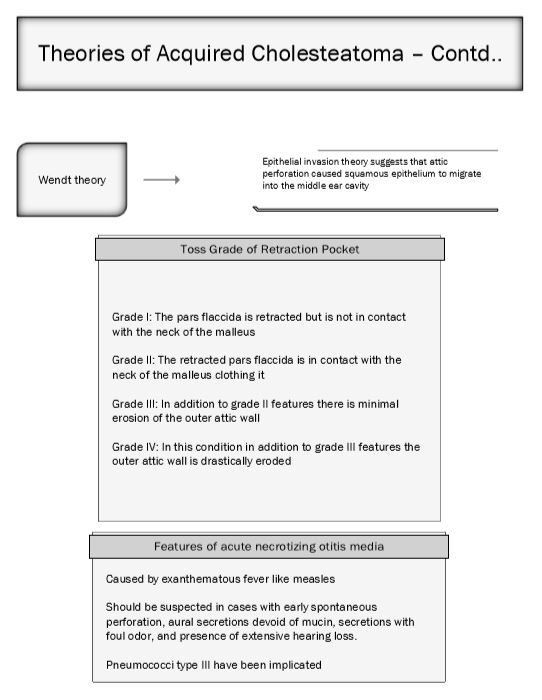
Theories of Active squamosal COM:
Cholesteatoma can also be classified according to its topology:
Attic cholesteatoma - This is actually a mixture of retraction pocket and papillary proliferation from the basal cell layer of squamous epithelium of pars flaccida.
Sinus cholesteatoma - This is a posteriosuperior retraction / perforation of pars tensa extending into the sinus tympani, posterior tympanum and beyond.
Tensa cholesteatoma - This is retraction and adhesion of the entire pars tensa and could involve tympanic orifice of eustachean tube.
Proliferation rate of cholesteatoma in comparison with that of skin lining of external canal is found to be 2.5 times higher. Defects in regulation of epidermal growth factor receptor system have also been identified in these patients. Current studies reveal that cholesteatoma arises from ear drum and not from skin lining of external canal / attic mucosa. This could account for the presence of cholesteatoma behind intact ear drum which has been classified under congenital cholesteatoma. Current literature does not acknowledge this condition as it is not a true congential disorder and does not fulfil the criteria for congenital disorders.
Congenital cholesteatoma:
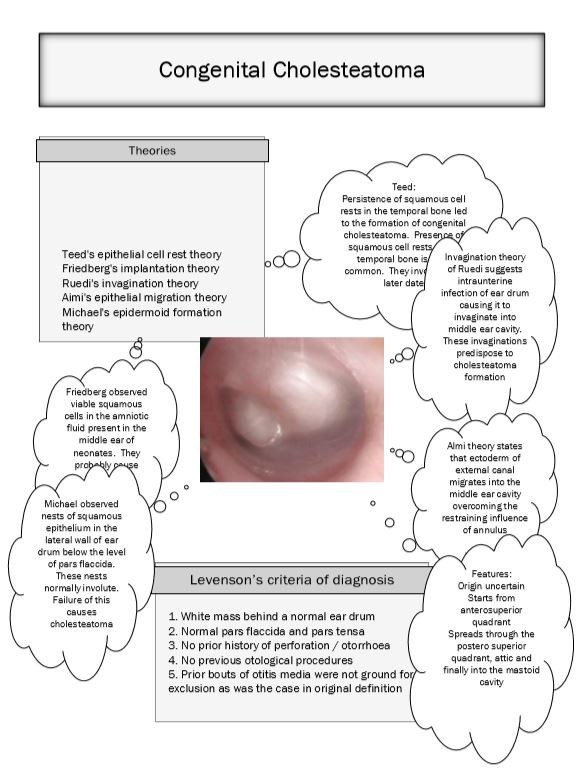
Even though this condition is currently not accepted this is included for the sake of completeness of the topic.
This condition is known to arise from embryonic cell rests present in the middle ear cavity and temporal bone. These cell rests are known to commonly occur in cerebello pontine angle and petrous apex. Infact congenital cholesteatoma is seen as a whitish mass behind an intact tympanic membrane.
Derlacki and Clemis laid down the following as criteria to diagnose congenital cholesteatoma:
1. The patient should not have previous episodes of middle ear disease
2. Ear drum must be intact and normal
3. It is purely an incidental finding
4. If discharge and ear drum perforation is present then it should be contrued that congential cholesteatoma has managed to erode the tympanic membrane.
Clinical features: The disorder is an incidental finding. The common location of congenital cholesteatoma is the antero superior quadrant of tympanic membrane, postero superior quadrant being the next common site of involvement. Anteriorly situated congenital cholesteatomas are known to affect the eustachean tube function causing conductive deafness due to middle ear effusion, where as posterior congenital cholesteatoma is known to cause conductive deafness due to impairment of ossicular chain mobility.
Staging of congenital cholesteatoma:
Staging as suggested by Derlacki and Clemis: They were the first to stage congenital cholesteatoma. They classified congenital cholesteatoma into
1. Petrous pyramid cholesteatoma
2. Cholesteatoma involving the mastoid cavity
3. Cholesteatoma involving the middle ear cavity.
Potsic suggested the following staging mechanism:
Stage I : Single quadrant involvement with no ossicular / mastoid involvement.
Stage II : Multiple quadrant involvement with no ossicular / mastoid involvement
Stage III : Ossicular involvement without mastoid involvement
Stage IV : Mastoid extension
Nelson's staging:
Type I : Involvement of mesotympanum without involvement of incus / stapes
Type II : Involvement of mesotympanum / attic along with erosion of ossicles without extension into the mastoid cavity
Type III : Involvement of mesotympanum with mastoid extension
Staging this disease will help in deciding the modality of treatment and in predicting the long term prognosis.
Healed COM:
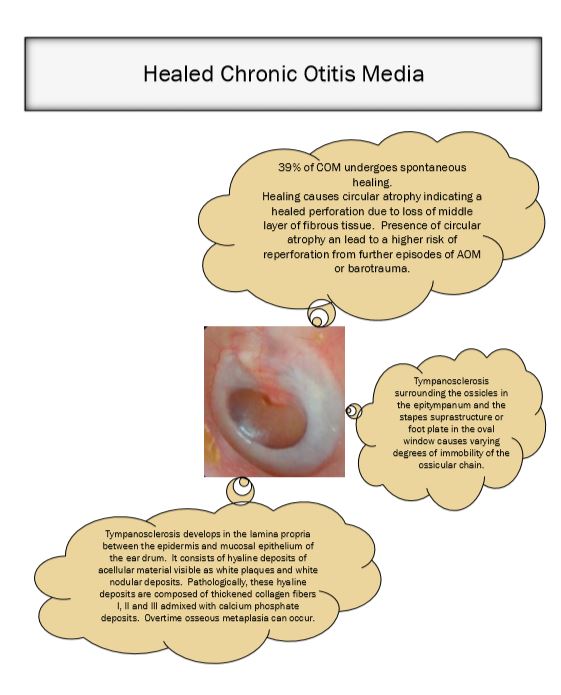
Nearly a quarter of patients with COM can undergo spontaneous healing. These patients show circular atrophy of ear drum indicating healed perforation. The presence of circular atrophy of ear drum could predispose it for reperforation due to further episodes of AOM / barotrauma. Other abnormalities found in the ear drum that could indicate healed com include tympanosclerosis.
Tympanosclerosis:
Is deposition of acellular hyaline and calcium deposits within the submucous layer of the tympanic membrane / submucous membrane of the middle ear cavity. In a majority of patients these plaques are so insignificant that they cause very little impairment in the hearing ability of the patient. These plaques could be likened to healed scar tissue.
When present over the tympanic membrane these plaques appear like a whitish cresentic shaped plaques.
Causes:
1. Could be caused by resolved otitis media.
2. Trauma
3. Chronic otitis media with effusion
4. After recurrent bouts of acute otitis media (middle ear tympanosclerosis)
5. After grommet insertion
6. Eustachean tube obstruction
