Pathology
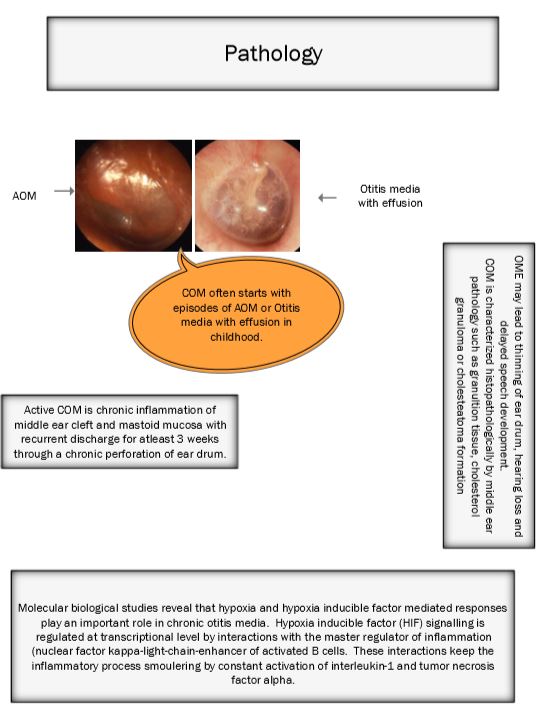
It is an accepted fact that chronic otitis media commonly starts with episodes of acute otitis media (AOM) or otitis media with effusion (OME) in childhood. OME leads to thinning of ear drum, hearing loss and delayed speech development.
COM can be characterized histopathologically by middle ear pathology like granulation tissue, cholesterol granuloma or cholesteatoma formation.
Active COM is chronic inflammation of middle ear / mastoid mucosa with recurrent discharge of atleast 2 weeks through chronic perforation of the ear drum.
Otitis media and chronic otitis media are multifactorial diseases involving no single genetic defect making it impossible to identify the single offending gene. Patient factors also play an important role in pathogenesis of COM. These factors include:
1. Innate immunity of the patient to the disease (toll-like receptors, cytokines and surfactants). Toll like receptors are pattern recognition receptors that are involved in the innate immune system against microbes. Toll like receptor 4 responds to and recognizes the lipopolysaccharide of gram negative bacteria. The innate immune system is the first line of defence against gram negative infections of middle ear cavity.
2. Adaptive immunity of the patient (Immunoglobulins)
3. Non specific immunity (presence of epithelial barriers and mucin production)
4. Inflammation regulation
5. Craniofacial abnormalities
Otitis media is cuaed by bacteria entering via the Eustachean tube. At this point it should be stressed that sterile otitis media is not that uncommon and initiation of inflammation in this scenario is rather unclear.
Various genetic models used to study pathogenesis of COM demonstrated hypoxia and hypoxia inducible factor (HIF) could be the mechanism involved in chronic inflammatory process of middle ear mucosa. HIF signalling is regulated at the transcriptional level by interactions with the master regulator of inflammation Nuclear factor kappa-light-chain-enhancer of activated B cells. At the translational level it is regulated by cytokines which are glycoproteins produced by inflammatory cells and epithelial cells like interleukin-1 amd TNF alpha.
Nuclear factor kappa-light-chain-enhancer can be activated by many factors they include:
Cytokines
Bacterkal lipopolysaccharides
Viral pathogens
Growth factors
Vascular endothelial growth factor also has been postulated to play a role in OME. Hypoxia drives inflammation by activation of Nuclear factor kappa-light-chain-enhancer, Interleukin-1 beta and Tumor necrosis factor-alpha increases angiogenisis, vascular permeability and recruitment of neutrophils through activation of vascular endothelial growth factor. Introduction of tymponostomy tubes (grommet) improves oxygenation of middle ear cavity downgrading IHF signalling.
Recruitment of inflammatory cells (neutrophils, mast cells, lymphocytes, plasma cells or monocytes/macrophages are integral to the initiation of chronic inflammation of middle ear mucosa. Once the inflammation has been initiated, there is accumulation of fluid and inflammatory cells in the middle ear cavity causing conductive deafness and rarely sensorineural hearing loss due to diffusion of cytokines through the round window membrane. Permeability of round window membrane is increased during the inflammatory process.
TNF-alpha and Interleukin-8 increase inducible nitric oxide synthase in the middle ear mucosa. Nitric oxide stimulates mucin production.
