Difference between revisions of "Myringoplasty"
| Line 89: | Line 89: | ||
Step V: | Step V: | ||
| − | Placement of graft (underlay technique). Now a properly dried temporalis fascia graft of appropriate size is introduced through the ear canal. The graft is gently pushed under the tympano meatal flap which has been elevated. The graft is insinuated under the handle of malleus. The tympano meatal flap is repositioned in such a way that it covers the free edge of the graft which has been introduced. Bits of gelfoam is placed around the edges of the raised flap. One gel foam bit is placed over the sealed perforation. This gelfoam has a specific role to play. Due to the suction effect created it pulls the graft against the edges of the perforation thus preventing medialisation of the graft material. | + | Placement of graft (underlay technique). Now a properly dried temporalis fascia graft of appropriate size is introduced through the ear canal. The graft is gently pushed under the tympano meatal flap which has been elevated. The graft is insinuated under the handle of malleus. The tympano meatal flap is repositioned in such a way that it covers the free edge of the graft which has been introduced. Bits of gelfoam is placed around the edges of the raised flap. One gel foam bit is placed over the sealed perforation. This gelfoam has a specific role to play. Due to the suction effect created it pulls the graft against the edges of the perforation thus preventing medialisation of the graft material.. |
Latest revision as of 10:49, 4 April 2020
Contents
Synonyms:
Myringoplasty, Tympanoplasty.
Definition:
Myringoplasty is a procedure used to seal a perforated tympanic membrane using a graft material.
Temporalis fascia is the commonly used graft material because:
1. It is an autograft with excellent chance of take
2. It is available close to the site of operation making its harvest easier
3. It has a low basal metabolic rate, brightening its success rate
4. Its thickness is more or less similar to that of tympanic membrane
There are two available methods of performing myringoplasty:
Overlay technique
Under lay technique
Overlay technique:
This is a difficult technique to master. Here the graft material is inserted under the squamous (skinlayer) of the ear drum. It is a difficult task peeling only the skin layer away from the tympanic membrane, placing the graft over the perforation and redraping the skin layer.
Underlay technique:
This is a simpler and commonly used technique. Here the graft is placed under the tympano meatal flap which has been elevated hence the name under lay. The major advantage of this procedure is that it is easy to perform with a good success rate.
Indications of Myringoplasty:
1. Central perforation which has been dry atleast for a period of 6 weeks.
2. As a follow up to mastoidectomy procedure to recreate the hearing mechanism
Prerequisites for myringoplasty:
1. Central perforation which has been dry for atleast 6 weeks
2. Normal middle ear mucosa
3. Intact ossicular chain
4. Good cochlear reserve
Procedure:
Firstly a temporalis fascia of adequate site must be harvested and allowed to dry. The surgery is performed under local anesthesia. Temporalis fascia graft is harvested under local anesthesia conventionally and allowed to dry. The external auditory canal is then anesthetised using 2 % xylocaine mixed with 1 in 10,000 adrenaline injection. About 1/2 cc is infiltrated at 3 - o clock, 6 - o clock, 9 - o clock, and 12 - o clock positions about 3mm from the annulus. The patient is premedicated with intramuscular injections of 1 ampule fortwin and 1 ampule phenergan.
Step I:
Freshening the margins of perforation - In this step the margins of the perforation is freshened using a sickle knife of an angled pick. This step is very important because it breaks the adhesions formed between the squamous margin of the ear drum (outer layer) with that of the middle ear mucosa. These adhesions if left undisturbed will hinder the take up of the neo tympanic graft. This procedure will infact widen the already present perforation. There is nothing to be alarmed about it.
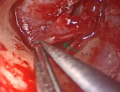
Step II:
This step is otherwise known as elevation of tympano meatal flap. Using a drum knife a curvilinear incision is made about 3 mm lateral to the annulus. This incision ideally extends between the 12 - o clock, 3 - o clock, and 6 - o clock positions in the left ear, and 12 - o clock, 9 - o clock and 6 - o clock positions in the right ear. The skin is slowly elevated away from the bone of the external canal. Pressure should be applied to the bone while elevation. This serves two purposes:
1. It prevents excessive bleeding
2. It prevents tearing of the flap
This step ends when the skin flap is raised up to the level of the annulus.
Step III:
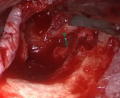
Elevation of the annulus and incising the middle ear mucosa. In this step the annulus is gradually lifted from its rim. As soon as the annulus is elevated a sickle knife is used to incise the middle ear mucosal attachment with the tympano meatal flap. This is a very important step because the inner layer of the remnant ear drum is continuous with the middle ear mucosa. As soon as the middle ear mucosa is raised, the flap is pushed anteriorly till the handle of the malleus becomes visible.
Step IV:
Freeing the tympano meatal flap from the handle of malleus. In this step the tymano meatal flap is freed from the handle of malleus by sharp dissection of the middle ear mucosa. Sometimes the handle of the malleus may be turned inwards hitching against the promontory. In this scenario, an attempt is made to lateralise the handle of the malleus. If it is not possible to lateralise the handle of the malleus, the small deviated tip portion of the handle can be clipped. The handle of the malleus is freshened and stripped of its mucosal covering.
Step V:
Placement of graft (underlay technique). Now a properly dried temporalis fascia graft of appropriate size is introduced through the ear canal. The graft is gently pushed under the tympano meatal flap which has been elevated. The graft is insinuated under the handle of malleus. The tympano meatal flap is repositioned in such a way that it covers the free edge of the graft which has been introduced. Bits of gelfoam is placed around the edges of the raised flap. One gel foam bit is placed over the sealed perforation. This gelfoam has a specific role to play. Due to the suction effect created it pulls the graft against the edges of the perforation thus preventing medialisation of the graft material..

Large central perforation

Perforated edges freshened with sickle knife

Endomeatal incision to elevate tympanomeatal flap

Endomeatal incision to elevate tympanomeatal flap
Middle ear entered. Arrow shows the middle ear cavity
Handle of malleus freshened with sickle knife
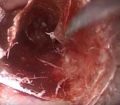
Temporalis fascia graft being introduced

Graft introduced under malleus handle. Arrow indicates the malleus handle

Graft sealing the perforation








